Experts said the same thing about germ theory, penicillin and peppermint oil that they now say about AI.
It is the Semmelweis reflex, and it is quietly opening a first-mover window for the credentialed practitioners who choose to be visible rather than invisible.
By James Burgin, founder of Thriving Practitioners and Brandwithin. Last reviewed June 2026.
In 1847, a young Hungarian doctor worked out something that should have been celebrated immediately. Ignaz Semmelweis noticed that women whose babies were delivered by doctors died of childbed fever far more often than women delivered by midwives.
He realised the doctors were carrying something deadly on their hands, straight from the autopsy room to the delivery ward. When he introduced handwashing with a chlorine solution, deaths on his ward fell from around 18 per cent to under 2 per cent (Science History Institute).
He had the data. He had the bodies to prove it.
The medical establishment ridiculed him. The idea that respectable physicians were the cause of death offended the profession’s sense of itself.
Semmelweis was pushed out, mocked, and eventually committed to an asylum, where he died in 1865, reportedly from the very kind of infection he had spent his life fighting (NPR). Vindication came only years later, once Louis Pasteur’s germ theory proved he had been right all along.
Hold that story in your mind, because there is a wave of confident voices declaring that artificial intelligence will fail!
Natural health practitioners are the people who should recognise this pattern fastest. Not because AI is the equal of penicillin. It is not, and it would cheapen the comparison to pretend otherwise.
But because the social pattern, the way good ideas are dismissed by credible experts right up until they become the standard, is identical. And our natural health profession has been on both sides of it.
Key Takeaways: AI for Natural Health Practitioners
- Patients Already Switched – One in three adults now ask AI health questions, so practitioners absent from AI answers are invisible to them.
- The Semmelweis Reflex – Every medical breakthrough was dismissed before adoption; AI faces the same reflex, and natural health has been vindicated repeatedly.
- Become The Cited Source – AI rewards credentialed, well-cited, genuinely useful content, so practitioners can become the trusted source AI recommends to patients.
- First-Mover Window – Natural health is among the slowest sectors to adopt AI, so practitioners moving now hold authority that latecomers struggle to displace.
The argument in one paragraph
Almost every transformative medical advance was first declared a failure, a fraud, or a fad by the leading authorities of its day.
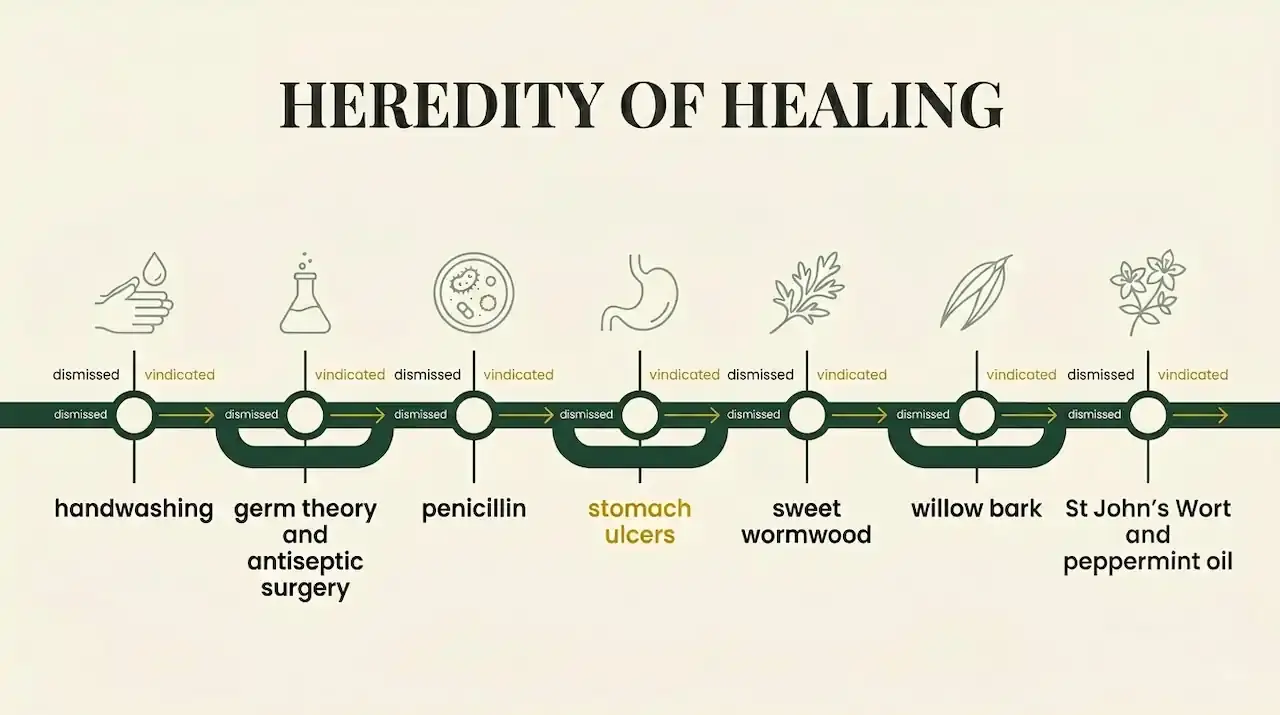
Handwashing, germ theory, antiseptic surgery, penicillin, and the bacterial cause of stomach ulcers were all dismissed, sometimes for decades, while patients paid for the delay.
The same reflex is now aimed at AI. Meanwhile, AI has quietly become the front door to health information for roughly a third of adults, and the natural health sector is among the slowest of any industry to adapt.
For a credentialed practitioner, that gap is not a reason to wait. It is a first-mover window that closes a little more every month.
A list of confident, catastrophic, wrong predictions
The marketer Ruben Hassid recently assembled a long catalogue of expert predictions that aged terribly.
- The telephone had “too many shortcomings to be seriously considered as a means of communication.”
- The home computer had “no reason” to exist.
- The iPhone had “no chance” of meaningful market share.
Each prediction came from someone with credentials, standing, and every reason to be taken seriously at the time.
What makes the list uncomfortable is that the people making the predictions were not fools. They were experts, reasoning carefully from the world they already knew.
Their error was almost never about the technology itself. It was about imagination. They could not picture the world the new thing would create, so they assumed that world would not arrive.
Hassid closes on a line that belongs on every practitioner’s desk this year:
“History does not repeat itself, but the people betting against it do.”
Healthcare has its own version of that list, with stronger feelings than for any gadget, because in medicine, the cost of dismissing a good idea is counted in lives.
Healthcare’s own catalogue of “this will fail”
Handwashing, and the bias that now bears its name
We have already met Semmelweis. What matters most is the aftermath.
The tendency to reject new evidence because it contradicts established beliefs is now a recognised cognitive bias, formally known as the “Semmelweis reflex” (Hajar, 2020, PubMed).
The man was right. The establishment was wrong. The only thing ever in question was how many people would die before the profession updated its beliefs.
Germ theory and antiseptic surgery
When Joseph Lister applied Pasteur’s germ theory to surgery in the 1860s, cleaning wounds and instruments with carbolic acid, mortality in his surgical ward fell sharply (Britannica).
British surgeons resisted his methods for the better part of two decades. Germ theory itself, the foundation of essentially all modern medicine, was treated as a fringe proposition before it became bedrock (Science Museum, London).
Penicillin, ignored for over a decade
Alexander Fleming observed in 1928 that a mould killed bacteria in his laboratory. The discovery sat largely unused for roughly twelve years until Howard Florey and Ernst Chain turned it into a usable drug at the start of the 1940s (American Chemical Society).
Antibiotics are credibly estimated to have saved on the order of 200 million lives since (National Library of Medicine). The single most consequential drug in human history spent more than a decade as a curiosity that nobody acted on.
Stomach ulcers, and an Australian who drank bacteria to prove a point
This one is recent enough to be a warning rather than a museum piece, and it is ours. In 1982, the Western Australian doctors Barry Marshall and Robin Warren proposed that most stomach ulcers were caused by a bacterium, Helicobacter pylori, not by stress and acid.
The idea was so far outside accepted thinking that Marshall’s early work was dismissed, and he struggled to be taken seriously (Lasker Foundation).
To prove it, he drank a culture of the bacteria himself, developed gastritis, and demonstrated the link directly. In 2005 he and Warren won the Nobel Prize in Physiology or Medicine (NobelPrize.org).
The lesson for anyone who has ever been dismissed for an unfashionable position is direct. The consensus is not the same thing as the truth, and the gap between them is exactly where good practitioners have always lived.
Sweet wormwood, and a Nobel Prize hiding in a 1,600-year-old text
Here is the story our profession should carry into every conversation about AI.
In the 1970s, the Chinese scientist Tu Youyou combed through ancient herbal texts in search of a malaria treatment, found a remedy using sweet wormwood in a roughly 1,600-year-old manuscript, and extracted the compound artemisinin from it.
That plant-based discovery now saves well over a hundred thousand lives a year, and in 2015 it won her the Nobel Prize in Physiology or Medicine (NobelPrize.org). Ancient wisdom. Validated by modern method. Resisted, doubted, and then proved profoundly right.
If anyone on earth should understand that the establishment is often wrong about what counts as legitimate, it is a natural health practitioner.
Willow bark, and the folk remedy that became the world’s most-used medicine
For centuries, people across the ancient world used willow bark for pain and fever. Then, by the early modern period in Europe, willow was largely dismissed as a serious medicinal option (The Conversation).
It took the curiosity of an English clergyman, Edward Stone, who reported his results to the Royal Society in 1763, to bring it back to scientific attention. Chemists later extracted its active compound, salicin, and refined it into the drug we now call aspirin, which Bayer named in 1899 (Science History Institute).
A traditional plant remedy, written off by the establishment of its day, became one of the most widely used medicines in human history.
St John’s Wort, and a folk tonic the regulator now takes seriously
St John’s Wort was for generations a folk remedy for low mood, exactly the kind of traditional plant medicine that modern science was inclined to wave away as unproven. The evidence eventually said otherwise.
A Cochrane systematic review, the most rigorous standard in evidence-based medicine, concluded that the extracts tested were superior to placebo in patients with depression and similarly effective to standard antidepressants, with fewer side effects, for mild to moderate cases (Cochrane, 2008).
The credibility marker is this: Australia’s Therapeutic Goods Administration does not dismiss it. The regulator treats it as a recognised active substance and publishes formal guidance for health professionals on its use and its interactions (Therapeutic Goods Administration).
When the country’s most rigorous medicines regulator writes the safety sheet for a herb once dismissed as folklore, the folklore has been vindicated.
Peppermint oil, and the remedy the specialists came around to
Peppermint oil is one of the oldest digestive remedies, and for a long time, the conventional view was that it lacked sufficient evidence to be taken seriously for conditions like irritable bowel syndrome. The careful work changed that view.
A meta-analysis of twelve randomised trials covering 835 patients found peppermint oil significantly improved global symptoms compared with placebo (Alammar et al., 2019, BMC), and the American College of Gastroenterology’s 2021 clinical guideline now formally suggests peppermint to provide relief of overall IBS symptoms (Lacy et al., ACG Clinical Guideline, 2021).
The specialists came around. That is the pattern this whole article is about. An old remedy is dismissed, the evidence is built patiently, and the establishment quietly adopts the position it once rejected.
The same pattern is playing out right now with AI, and the practitioners who recognise it early will be cited as the trusted source, while everyone else is still arguing about whether it is real.
The reflex is now pointed at AI
The same reflex that rejected handwashing now targets artificial intelligence, and the arguments follow the familiar pattern.
- The cognitive scientist Noam Chomsky called large language models “the false promise of ChatGPT” (The New York Times).
- The novelist Ted Chiang described them as “a blurry JPEG of the web,” compressing and degrading real knowledge (The New Yorker).
- Goldman Sachs published a widely read note asking whether generative AI was “too much spend, too little benefit” (Goldman Sachs).
- The Nobel laureate economist Daron Acemoglu has argued that AI’s effect on productivity will be modest (Fortune).
These are serious people making serious arguments, exactly as the doubters of germ theory were serious people.
And here is the part that matters for a clinic owner. Even if every one of them is correct on their own terms, none of their arguments is a reason for a practitioner to wait.
Read carefully, each one is actually an argument for moving now.
Read the sceptics as instructions, not warnings

Ted Chiang is right, and it is the best news in this article. If AI is a “blurry JPEG” that compresses the web, then the quality of what it produces depends entirely on the quality of the source material it compresses from.
A clinic with thin, generic, uncited content becomes a blurry copy of a blurry copy.
A clinic with deep, credentialed, well-cited content becomes the sharp source image that the AI reaches for.
Chiang’s critique is not a reason to ignore AI. It is a brief for becoming the highest-quality source in your niche.
Goldman Sachs is talking about a different problem than yours. Their concern is whether trillion-dollar capital expenditure by technology giants pays off at the macro level.
That is a real and open question for investors. It has almost nothing to do with whether a naturopath benefits from a tool that helps draft a newsletter, or makes their clinic findable when a patient asks an AI assistant for help.
The macro debate about spending does not change the micro reality that the tools already work and are already in your patients’ hands.
Acemoglu’s caution is itself the strategy. His central point is that AI delivers value when it augments human expertise rather than replacing it. That is precisely the posture a credentialed practitioner should take.
You are not asking AI to be the clinician. You are using it to extend the reach of your clinical judgement, to draft, to structure, and to make your genuine expertise discoverable.
Applied to a clinic, the Nobel laureate’s warning reads as an endorsement.
The doubters of germ theory were not wrong because they were stupid. They were wrong because they mistook the limits of the early evidence for the limits of the idea.
The AI sceptics are making a more sophisticated version of the same mistake.
Why this matters now, not later

While the debate continues, patient behaviour has already moved.
One in three adults now use an AI chatbot for health information. In Rock Health’s 2025 consumer survey of 8,000 adults, the figure reached 32 percent, double the 16 percent recorded a year earlier (Rock Health, 2026). Closer to home, a nationally representative study published in the Medical Journal of Australia found that around one in ten Australian adults had used ChatGPT for health information in the six months to mid 2024, which the authors estimated at roughly 1.9 million people (Ayre et al., MJA, 2025).
Search itself has changed shape. By late 2025, Google was showing an AI Overview on 89 per cent of healthcare-related queries, up from 59 per cent two years earlier (BrightEdge, 2025). When an AI summary appears, users are far less likely to click through to a website, with click-through rates falling from around 15 per cent to 8 per cent (Pew Research Centre, 2025).
The practical consequence is stark. If your clinic is not the source the AI cites, you are increasingly invisible at the exact moment a patient is looking for help.
The revealing exception in this data – Local Search
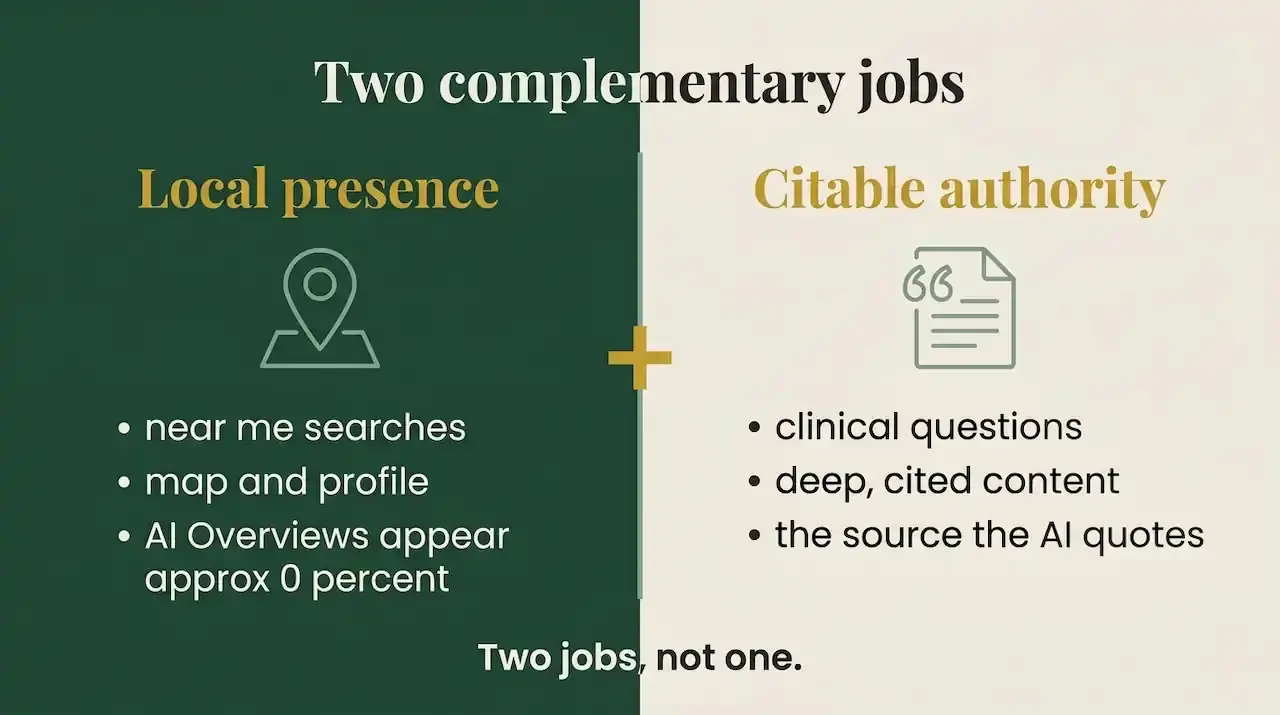
For local “near me” queries, AI Overviews appeared essentially zero per cent of the time, down from full coverage two years earlier (BrightEdge, 2025).
Local intent still goes to the map and the practitioner profile. That means your local presence and your citable-authority content are two distinct and complementary roles, not one.
The first-mover window is specific to this sector
Here is where history turns into opportunity.
The natural health sector is among the slowest to adopt these tools, with Australian small-business surveys showing the sector lagging well behind industries like marketing, and sole traders even slower still (BizCover, 2025).
That gap is the opportunity.
When patient demand has already shifted to AI, but practitioner adoption has not, the practitioners who move first, capture authority that is expensive for latecomers to dislodge.
The doctors who washed their hands early did not have to fight for the position once it became standard. They simply held it.
The same is true of citable authority in an AI-mediated search environment. The clinic that becomes the trusted source in its niche this year is the one the AI models keep returning to next year.
In our work building and coaching about authority sites for natural health practitioners, the pattern is consistent. The clinics that win the AI-search era are not the ones with the biggest budgets.
They are the ones whose content is the most credentialed, the most carefully cited, and the most genuinely useful, because that is exactly what the models are built to reward.
James Burgin, Thriving Practitioners
What does becoming a citable source actually require?
Becoming the source an AI cites is not luck, and it is not volume.
The research on generative engine optimisation (GEO) is specific about what works.
The foundational study from Princeton, Georgia Tech, the Allen Institute for AI, and IIT Delhi found that adding relevant statistics, expert quotations, and citations to credible sources measurably increased the likelihood of content being cited by AI, with statistics alone lifting visibility by up to around 40 per cent, while crude keyword stuffing reduced it (Aggarwal et al., 2024, arXiv).
Notably, the same body of research finds that ranking first on Google has only a weak relationship with being cited by AI.
The old game of chasing the top blue link is not the same as the new game of being the trusted source. What the models reward is precisely what credentialed practitioners are naturally positioned to provide: genuine expertise, real data, clear attribution, and information that adds something the rest of the web does not.
This is the same standard we teach inside Pathway to Practice Visibility, our on-demand program that takes a practitioner from invisible to the expert AI recommends.
Doing this safely and within the rules
For Australian practitioners, AI is a tool, not a shortcut around professional obligations. The Therapeutic Goods Administration’s advertising rules and the Australian Health Practitioner Regulation Agency’s restrictions on testimonials apply in full to anything you publish, regardless of whether a person or a machine drafted it.
There is no AI-specific carve-out and no AI-specific exemption. As of mid 2026, the safe assumption is the strict one. You remain fully accountable for every claim, and AI-drafted copy must be reviewed against the same compliance standard as anything you write yourself.
Used this way, with qualifying language, no diagnostic or curative claims, and a human clinician’s review on everything, AI extends your reach without expanding your risk.
What to do next – your action steps
- Audit how your clinic currently appears when a patient asks an AI assistant about your area of practice. Type the real questions your patients ask into ChatGPT, Perplexity, and Google’s AI Overview, and see whether you are cited, mentioned, or absent.
- Identify the handful of questions in your niche where being the cited source would matter most, usually your highest-intent clinical topics.
- Build genuinely authoritative content on those topics, with real statistics, named credible sources, and your own expert commentary, to the standard the models reward.
- Keep a human clinician’s review on everything, and check every published claim against TGA and/or AHPRA requirements before it goes live.
- Treat your local presence and your authority content as two separate jobs, because patients reach you through both, and AI currently behaves very differently for each.
A closing thought for brightness of the future
The history of medicine is, in large part, a history of good ideas that were dismissed before they were adopted.
Handwashing, germ theory, penicillin, the bacterial cause of ulcers, a Nobel Prize pulled from a 1,600-year-old herbal text, a folk tonic the medicines regulator now writes safety sheets for, and a digestive remedy the gastroenterologists came around to were all, at some point, positions that serious experts confidently declared wrong.
The practitioners who recognised the shift early did not just benefit personally. They moved the whole field forward.
A confident chorus is now declaring that AI will fail, while the behaviour it is supposed to fail at has already become normal for a third of the population.
Practitioners know all too well what it costs to be dismissed by people who are certain.
The danger is not that you will be dismissed again. The danger is that, this once, you will be the one doing the dismissing.
History does not repeat itself. But the people betting against it do. The only open question for your clinic is which side of that bet you would like to be on.
If you are ready to be on the right side of it, Pathway to Practice Visibility will show you exactly how, step by step, in your own authentic voice.
Frequently asked questions
Is AI going to replace natural health practitioners?
No. The evidence and the expert consensus point the other way. Economists who study AI argue that its value comes from augmenting human expertise, not replacing it (Fortune, 2026). Patients still want a credentialed human to make clinical decisions. AI changes how they find you, not whether they need you.
Why should I trust AI when respected experts say it will fail?
Respected experts have a long history of declaring transformative advances dead on arrival, from the telephone to the internet to, in medicine, germ theory and the bacterial cause of ulcers. Healthy scepticism is good, but the track record of confident predictions of failure is poor. The safer position is to watch what patients are actually doing, and a third of adults are already using AI for health information (Rock Health, 2026).
What is the Semmelweis reflex?
It is the documented tendency to reject new evidence or ideas because they contradict established beliefs, named after the physician whose proof that handwashing saves lives was rejected by the medical establishment of his day (PubMed, 2020). It is a useful lens for spotting when an idea is being dismissed for being unfamiliar rather than for being wrong.
How do AI assistants decide which health websites to cite?
Research on generative engine optimisation suggests AI systems favour content with relevant statistics, expert quotations, and citations to credible sources, and they penalise keyword stuffing (Aggarwal et al., 2024). Ranking first on traditional search has only a weak link to being cited by AI, so genuine authority and information value matter more than old-style optimisation.
Is it compliant for an Australian practitioner to use AI for marketing?
Using AI as a drafting and research tool is compatible with Australian rules, provided the output meets the same standards as anything else you publish. TGA advertising requirements and AHPRA’s restrictions on testimonials apply regardless of how content was created, and a clinician remains responsible for every published claim. As of mid 2026 there is no AI-specific exemption, so the strict standard applies.
Why act now rather than wait for the technology to settle?
Because patient behaviour has already moved while practitioner adoption has not. The Australian health sector lags well behind other industries in AI adoption (BizCover, 2025), which creates a first-mover window. Authority established now is difficult and expensive for latecomers to displace later.
References
- Science History Institute. Ignaz Semmelweis. https://www.sciencehistory.org/education/scientific-biographies/ignaz-semmelweis/
- NPR. The Doctor Who Championed Hand-Washing And Saved Women’s Lives. https://www.npr.org/sections/health-shots/2015/01/12/375663920/the-doctor-who-championed-hand-washing-and-saved-womens-lives
- Hajar R. The Semmelweis Reflex. PubMed, 2020. https://pubmed.ncbi.nlm.nih.gov/33437127/
- Encyclopaedia Britannica. Joseph Lister. https://www.britannica.com/biography/Joseph-Lister-Baron-Lister-of-Lyme-Regis
- Science Museum, London. Germ theory. https://www.sciencemuseum.org.uk/objects-and-stories/medicine/germ-theory
- American Chemical Society. Discovery and Development of Penicillin. https://www.acs.org/education/whatischemistry/landmarks/flemingpenicillin.html
- National Library of Medicine (PMC). Antibiotics and lives saved. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4378521/
- Lasker Foundation. Role of Helicobacter pylori in gastritis and peptic ulcer disease. https://laskerfoundation.org/winners/role-of-helicobacter-pylori-in-gastritis-and-peptic-ulcer-disease/
- The Nobel Prize. Barry J. Marshall, Facts. https://www.nobelprize.org/prizes/medicine/2005/marshall/facts/
- The Nobel Prize. Tu Youyou, Facts. https://www.nobelprize.org/prizes/medicine/2015/tu/facts/
- The New York Times. Noam Chomsky: The False Promise of ChatGPT. https://www.nytimes.com/2023/03/08/opinion/noam-chomsky-chatgpt-ai.html
- The New Yorker. ChatGPT Is a Blurry JPEG of the Web. https://www.newyorker.com/tech/annals-of-technology/chatgpt-is-a-blurry-jpeg-of-the-web
- Goldman Sachs. Gen AI: Too Much Spend, Too Little Benefit? https://www.goldmansachs.com/insights/top-of-mind/gen-ai-too-much-spend-too-little-benefit
- Fortune. Nobel laureate Daron Acemoglu on AI and productivity. https://fortune.com/2026/06/21/nobel-laureate-daron-acemoglu-ai-productivity-capitalism-democracy/
- Rock Health. Health AI insights from Rock Health’s 2025 Consumer Adoption Survey. https://rockhealth.com/insights/the-tortoise-and-the-hare-of-care-health-ai-insights-from-rock-healths-2025-consumer-adoption-survey/
- Ayre J, et al. Use of ChatGPT to obtain health information in Australia, 2024. Medical Journal of Australia, 2025. https://www.mja.com.au/journal/2025/222/4/use-chatgpt-obtain-health-information-australia-2024-insights-nationally
- BrightEdge. Healthcare and AI Overviews: How Google Sharpened Its Approach Over Three Years. https://www.brightedge.com/resources/weekly-ai-search-insights/healthcare-ai-evolution-google-2023-2025
- Pew Research Center. Google users are less likely to click on links when an AI summary appears. 2025. https://www.pewresearch.org/short-reads/2025/07/22/google-users-are-less-likely-to-click-on-links-when-an-ai-summary-appears-in-the-results/
- BizCover. How AI is transforming the Australian small business sector. 2025. https://www.bizcover.com.au/ai-transforming-australian-small-business-sector/
- Aggarwal P, et al. GEO: Generative Engine Optimization. arXiv, 2024. https://arxiv.org/abs/2311.09735
- The Conversation. Hippocrates and willow bark? What you know about the history of aspirin is probably wrong. https://theconversation.com/hippocrates-and-willow-bark-what-you-know-about-the-history-of-aspirin-is-probably-wrong-148087
- Science History Institute. Aspirin: Turn-of-the-Century Miracle Drug. https://www.sciencehistory.org/stories/magazine/aspirin-turn-of-the-century-miracle-drug/
- Cochrane. St John’s wort for treating depression. 2008. https://www.cochrane.org/evidence/CD000448_st-johns-wort-treating-depression
- Therapeutic Goods Administration. St John’s Wort: information sheet for health care professionals. https://www.tga.gov.au/safety/safety-monitoring-and-information/safety-alerts/st-johns-wort-information-sheet-health-care-professionals
- Alammar N, et al. The impact of peppermint oil on the irritable bowel syndrome: a meta-analysis of the pooled clinical data. BMC Complementary and Alternative Medicine, 2019. https://pmc.ncbi.nlm.nih.gov/articles/PMC6337770/
- Lacy BE, et al. ACG Clinical Guideline: Management of Irritable Bowel Syndrome. American Journal of Gastroenterology, 2021;116(1):17-44. https://pubmed.ncbi.nlm.nih.gov/33315591/
This article is general information for practitioners about marketing and discoverability. It is not clinical, legal, or regulatory advice. Practitioners are responsible for ensuring their own published content complies with TGA and AHPRA requirements. Written by James Burgin, Thriving Practitioners and Brandwithin. Last reviewed June 2026. This article is refreshed every six months.